
athenahealth
Control Through Interaction: Solving Interoperability Without Infrastructure Changes
How do you give clinicians visibility into incoming records without rebuilding the workflows they depend on?
My role & impact
I was the sole designer a scrum team tackling interoperability. I led research and design for this feature, which gives clinicians visibility into incoming documents before they're permanently added to the health record. My work resulted in user satisfaction increasing from 47% to 85%.
Team Make-up
Sole UX designer on a scrum team made up of 1 product manager, 1 engineering manager, and 4 developers.
Tools
Figma, pen & paper, Qualtrics, Mural
Timeline
~6 months for this portion of the work
The problem
Clinicians do not have transparency into how outside documents are categorized in patient health records, and no ability to manage what gets permanently added. This results in cluttered health records, wasted time hunting for relevant information, and added administrative burden. This compounds a well-established problem of clinician burnout, and in some cases, risks delays in care decisions.
The inability to easily find information led me to believe that there's a misalignment between the clinician mental model and how the organization/categorization system works.
I needed to understand mental models at this point and learn how clinicians conceptually organize or "bucket" documents.
From taxonomy to autonomy

There is a mismatch in how document categorization doesn't align with needs. Users document their own version of the information as seen in the internal note text box.
Through card sorting and contextual inquiry with clinicians, I validated a critical mismatch: automatic document categorization doesn't reflect how users mentally organize information.
Different clinical roles extract different data from the same document based on specialty and job-to-be-done.
Restructuring could theoretically improve findability, but the underlying infrastructure was externally owned and therefore, not feasible to change.
This constraint became the catalyst for reframing the problem. Instead of fixing taxonomy, I needed to give clinicians control at the interaction level.
Adding internal notes/tags, further user organization needed validation and dev input/research from a technical perspective. I shared this with the dev team and learned that it would be too much work to tackle the organization issue.
I explored which parts of the proposed workflow felt concrete, and identify which parts needed validation. I used this as an artifact to point to when discussing the feature idea, and potential paths forward after implementing the ability to preview and add, to consider the future of this work stream.
How much is enough? (Spoiler: all of it)
Low-fidelity designs and resonance testing with clinicians and research participants explored in-workflow document surfacing and information density.
To de-risk the design direction, I validated with a concept video and survey, combining qualitative and quantitative feedback in a lightweight, efficient approach.
Key insight: users wanted to see the full document in context with their current task to gauge relevance—partial previews weren't sufficient.
From here, I knew I was moving forward with the document preview/add functionality.
I needed to determine which parts of the workflow made sense to incorporate the new feature, and how much information needed to be surfaced.
Excitement around the preview idea
-
Easier to wade through the dozens (sometimes hundreds) of outside records without having to click to open them completely, only to find useless demographic pages
— physician
-
BEING ABLE TO PREVIEW THE DOCUMENT BEFORE IT IS ADDED TO THE CHART Would be AWESOME and SAVE so much time, energy and duplicate efforts. PLEASE ENABLE THIS FEATURE AS SOON AS POSSIBLE! …..
— Medical Assistant
-
...control over what is downloaded into the chart
EMR Manager
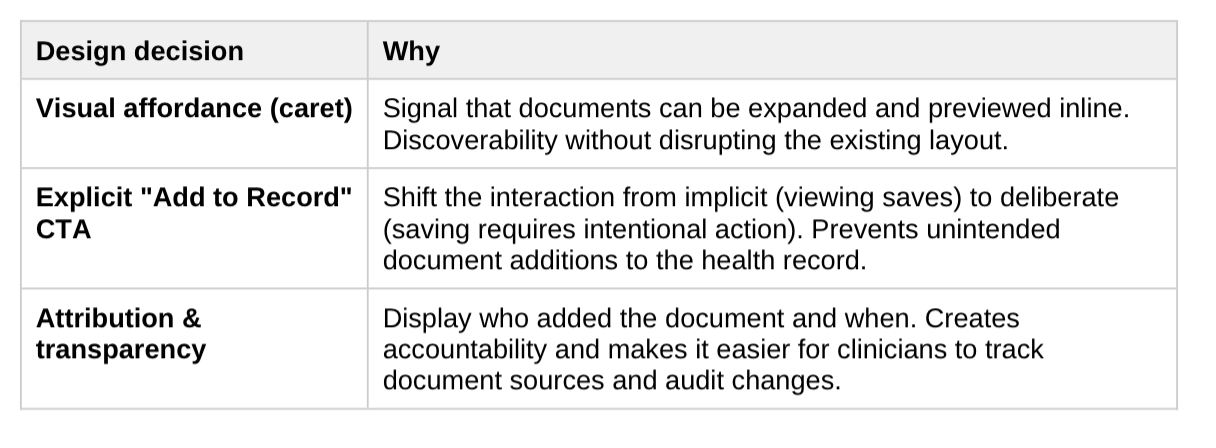
Moving from implicit to intentional
I made these design decisions knowing that we had to integrate this functionality within existing workflows.
Final Designs & Results
Users were able to identify clinically meaningful documents before adding. Downloads became more intentional and informed.
User satisfaction of finding/determining relevant documents
High-impact design often requires identifying the smallest viable intervention with systemic constraints. Taxonomy and restructuring remains a longer-term opportunity, however shifting the interaction model delivered value quickly and created a foundation for future evolution.